
New to Touchpoints180?
A metabolic psychiatry practice blending brain science, metabolism & education.
Our Story
The Book
Work With Us
Some sessions teach content. A rare few change how you think. And then there are the vanishingly rare ones — the kind that change how your brain holds the content, how your body remembers it, how your clinical instincts recalibrate without you consciously trying. That’s what happened during the solo afternoon brain health symposium led by Annette Bosworth, MD. It demonstrated how teaching becomes medicine. And it was, without exaggeration, the most effective medical teaching workshop I’ve ever experienced. Not just the most charismatic. Not the most credentialed. The most effective.
And the distinction matters.
She Didn’t Lecture. She Architected Learning.
From the moment the session began, it was clear this would not be passive. There were no long stretches of listening while slides advanced in the background. Instead, the room itself became the medium.
Flip charts appeared along the walls.
Large poster scorecards were taped up, ready to be filled.
Tables became working groups, not seating arrangements.
Hands were busy. Bodies were moving. Eyes were up.
At times, she posed provocative questions and asked us to commit publicly — not with raised hands, but with written answers, tallied responses, and visible group consensus. Other times, she turned learning into play: scratch tickets to reveal answers, games that required prediction before explanation, physical challenges that exposed cognitive limits instantly.
None of it felt gimmicky.
It felt intentional.
This was pedagogy designed by someone who understands the brain deeply enough to know that attention, novelty, movement, and social engagement are not add-ons to learning — they’re prerequisites.
Learning Was Made Physical — On Purpose
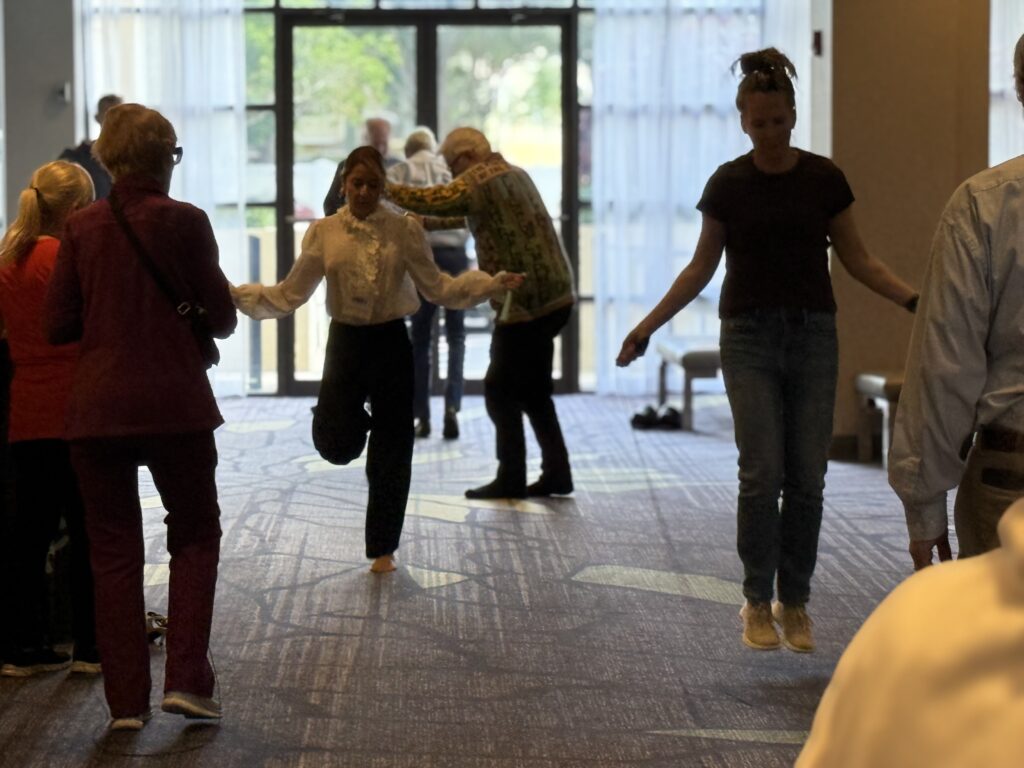
At one point, jump ropes came out.
Not metaphorically. Literally.
We were asked to jump. To coordinate. To track timing, rhythm, and error correction in real time. The room shifted — laughter, mild discomfort, sudden concentration. And then… almost immediately… insight.
This wasn’t about fitness.
It was about neurologic integration.
Balance. Timing. Working memory. Frustration tolerance. Autonomic regulation.
In seconds, abstract concepts about frontal lobe function, cerebellar coordination, and cognitive reserve became embodied knowledge. You didn’t need to memorize it. Your nervous system had already learned it. You were learning how teaching becomes medicine.
That was the genius of the session: she bypassed rote cognition and taught directly through experience.
The Brain Was Treated as a Structure, Not a Metaphor
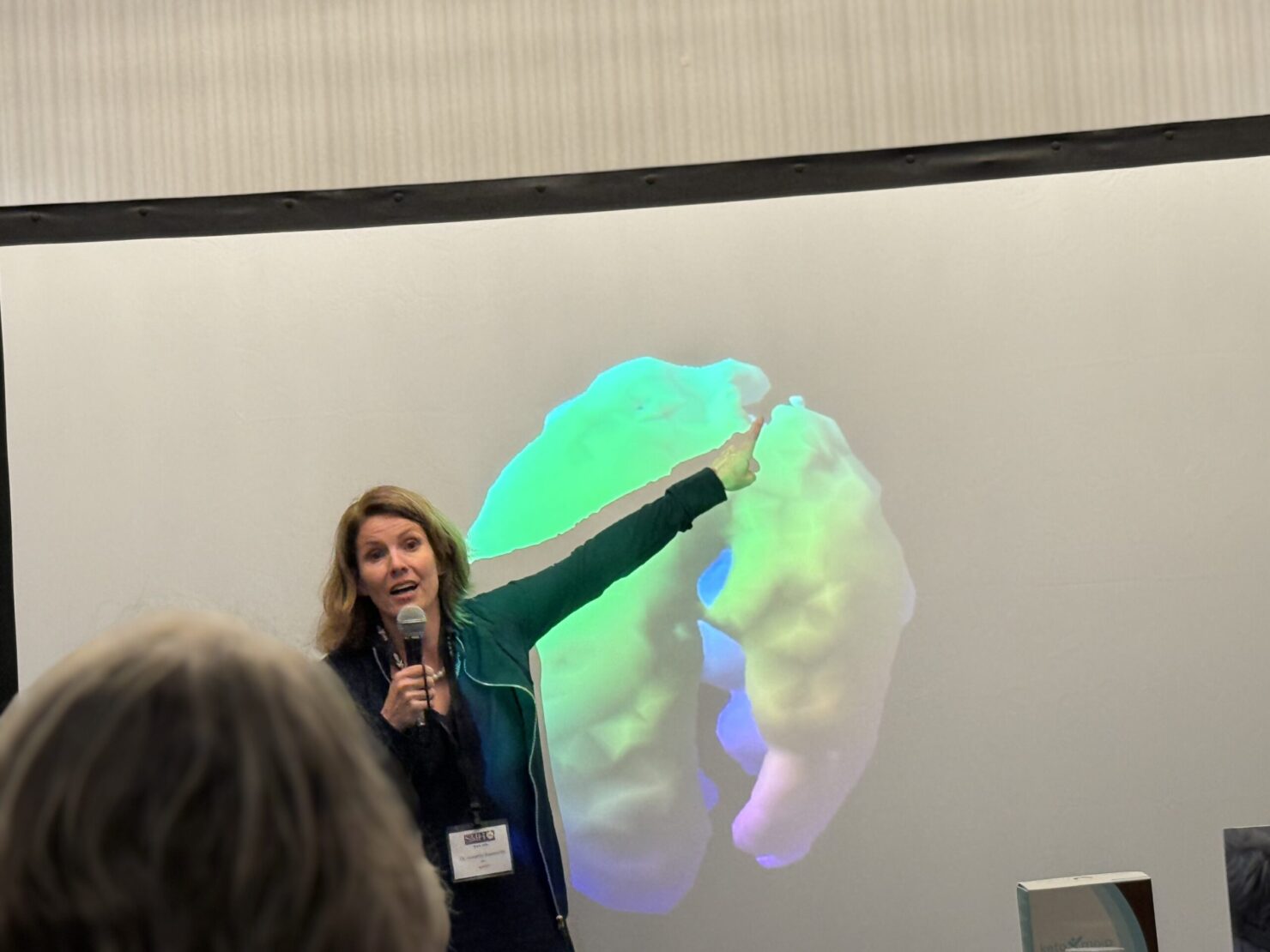
When she turned to neuroscience, it was never vague. The hippocampus was not an idea — it was a structure with volume, vulnerability, and timing. Brain development was not aspirational — it was time-sensitive, with windows that can be delayed, stalled, or reopened under the right conditions.

Using imaging, case examples, and storytelling, she showed how:
…Alcohol quietly shrinks critical brain regions long before anyone calls it addiction
…Sleep apnea suffocates cognition nightly while patients are told they’re “just tired”
…Iron deficiency and malnutrition masquerade as psychiatric illness
…Head injuries in adolescents derail emotional development for years
…Trauma arrests maturation in ways that look behavioral but are profoundly biological
Again and again, a sobering truth surfaced: many of the traits we judge most harshly are downstream of unrecognized brain injury.
And then — just as importantly — she showed what happens when those injuries are finally addressed.
Hope, Without Sentimentality
This was not a feel-good talk.
It was a hopeful one — but hope grounded in physiology, not optimism.
Brains can heal.
Volume can return.
Function can improve.
But only if the terrain allows it.
She was unflinching about the prerequisites: oxygen at night, inflammation reduced, metabolic chemistry stabilized, sleep protected, alcohol addressed, nutrition restored. Tools like TMS were discussed candidly — powerful, yes, but limited if the underlying metabolic and inflammatory environment remains hostile.
This was not magic.
It was conditions-based repair.
And it reframed failure — not as lack of effort, but as lack of readiness.

The Room Didn’t Just Learn. It Changed.
What stayed with me most was the collective effect.
This wasn’t a room full of individuals taking notes. It was a room thinking together.
Negotiating answers. Revising beliefs in real time. Building shared understanding through visible, iterative processes. Learning how teaching becomes medicine.
By the end, you could feel it: the content wasn’t just remembered — it was embedded.
Anchored in movement, emotion, conversation, and structure.
This is the kind of teaching that follows you back into clinic. That changes how you listen to patients. That makes you pause before labeling someone “resistant,” “noncompliant,” or “difficult.”
Because once you’ve seen how profoundly the brain shapes behavior — and how repair actually happens — you can’t unsee it.
A Final, Necessary Observation
She could have been teaching anywhere.
Hopkins.
Harvard.
Yale.
Her command of neuroscience, clinical medicine, behavior, and education easily belongs on those stages. But what made this session extraordinary wasn’t prestige.
It was respect for the learner.
Respect for how adults actually learn.
Respect for how brains actually change.
And respect for the difference between telling and transforming.
In a conference filled with outstanding science, this workshop stood apart — not because it was louder, but because it was alive.
And in the end, that may be the highest compliment we can give a teacher:
She didn’t just inform us.
She changed how our brains held the information.
That is teaching as medicine.
If this resonated with you
Here’s where to go next
Explore the Practice
Learn how we integrate psychiatry, metabolic medicine, and education into a coherent whole.

Read the Book
Toxic Roots — Dr. Calabrese’s guide to the biological forces reshaping our generation’s mental health.
Start a Conversation
A free 15-minute Discovery Call to explore whether our approach is right for you.
You Might Also Like
All Articles →

About the Author
Dr. Lori Calabrese, MD
Dr. Calabrese is a board-certified psychiatrist and metabolic medicine physician with over two decades of clinical experience. Her work sits at the intersection of brain health, metabolism, and patient education — helping individuals understand the biological roots of how they think, feel, and function.
She is the founder of Touchpoints180 and author of Toxic Roots, a physician’s guide to understanding the metabolic underpinnings of mental illness.
Ready to go deeper?
This conversation is where clarity begins.
If what you read here resonates — if you’ve sensed that your brain and body are trying to tell you something medicine hasn’t been able to translate — a Discovery Call is your first step.
Schedule a Discovery Call15 minutes. No commitment. Just conversation.

